Every month, a healthy ovary is supposed to release one mature egg — this is called ovulation. When that release doesn’t happen on schedule, or doesn’t happen at all, doctors describe it as one of several possible Ovulation Problems. This isn’t a single disease. It’s a broad term for anything that disrupts the timing or quality of egg release, and it’s one of the most common reasons women have trouble conceiving.
How Normal Ovulation Works
A normal cycle depends on a chain of signals between the brain and the ovaries. The hypothalamus and pituitary gland release hormones that tell the ovary to grow a follicle, and once that follicle matures, a surge in luteinizing hormone triggers the egg to be released. This whole process usually takes place around day 14 of a 28-day cycle, though it varies from woman to woman. After release, the empty follicle produces progesterone, which prepares the uterus lining for a possible pregnancy. If any step in this chain is interrupted, ovulation can be delayed, irregular, or skipped entirely.
How Ovulation Disorders Affect Fertility
When an egg isn’t released regularly, there’s simply no egg available for sperm to fertilize during that cycle. This is why doctors often check for Ovulation Problems early when a couple is trying to conceive without success. Even when ovulation does happen, poor timing or a weak hormonal follow-through can lower the chances of a fertilized egg implanting properly. The good news is that many of these issues can be identified with a few straightforward tests and often respond well to treatment.
Types of Ovulation Problems
Anovulation
Anovulation means no egg is released at all during a cycle. It’s often linked to conditions like PCOS, thyroid imbalances, or very low body weight, though sometimes no clear cause is found right away. Women with anovulation may still get periods, but these periods usually aren’t linked to true ovulation. Blood tests checking progesterone levels midway through the cycle are typically used to confirm this.
Oligo-ovulation
Oligo-ovulation refers to ovulation that happens, but infrequently — sometimes only a few times a year instead of monthly. Cycles tend to be long and unpredictable, which can make it hard to know when fertile days occur. This pattern is common in women with PCOS or in those going through significant weight changes. Tracking cycle length over a few months usually reveals this pattern clearly.
Luteal Phase Defect
This occurs when the second half of the cycle, after ovulation, is too short or doesn’t produce enough progesterone. Since progesterone is what prepares the uterus lining for implantation, a defect here can make it harder for a fertilized egg to attach and grow. Women with this issue often notice shorter cycles or spotting before their period is due. It’s typically diagnosed through hormone testing timed to the luteal phase.
Premature Ovarian Insufficiency (POI)
POI happens when the ovaries stop working normally before age 40, leading to reduced egg supply and irregular or absent periods. It’s different from menopause because some women with POI still ovulate occasionally and can conceive naturally or with treatment. Early signs include hot flashes, night sweats, and skipped periods in younger women. Blood tests measuring FSH and AMH levels help confirm this diagnosis.
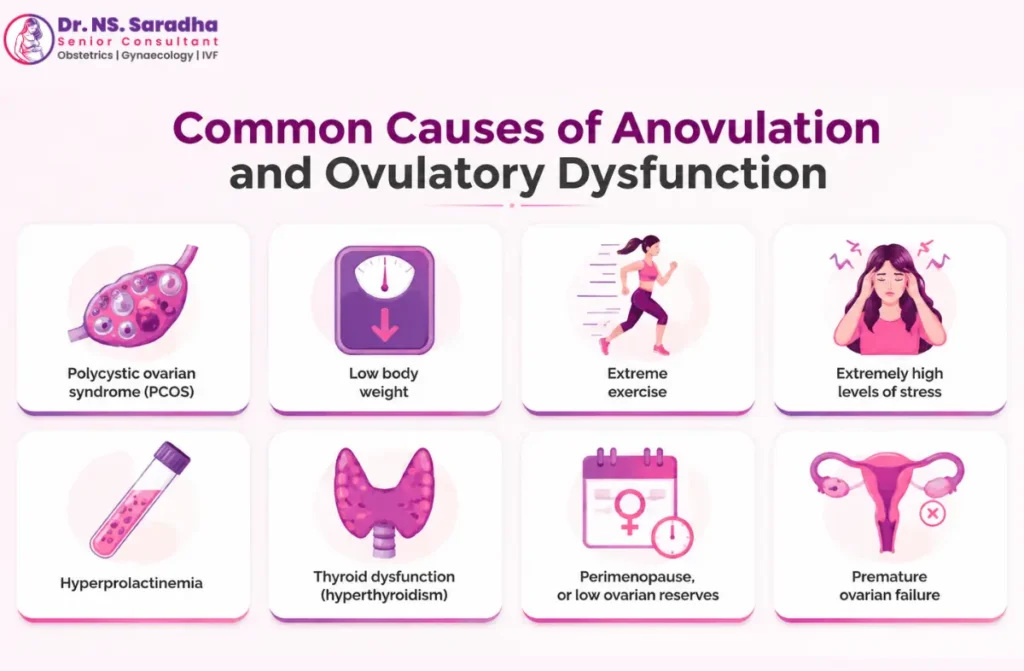
Common Causes of Ovulation Problems
Polycystic Ovary Syndrome (PCOS)
PCOS is one of the most frequent causes of irregular or absent ovulation. It involves a hormonal imbalance where the ovaries produce excess androgens, which can prevent follicles from maturing and releasing an egg properly. Many women with PCOS also experience weight gain, acne, or excess hair growth alongside irregular cycles. With the right combination of lifestyle changes and medication, ovulation can often be restored.
Hormonal Imbalances
Hormones like FSH, LH, estrogen, and progesterone all need to work in the right balance and sequence for ovulation to occur. Even small disruptions — from stress, illness, or certain medications — can throw this sequence off. This is one reason Ovulation Problems aren’t always tied to a single obvious cause. A detailed hormone panel usually helps pinpoint where the imbalance is happening.
Thyroid Disorders
Both an underactive and overactive thyroid can interfere with the hormonal signals needed for regular ovulation. The thyroid gland has a direct relationship with reproductive hormones, so even mild thyroid dysfunction can cause noticeable cycle changes. Many women don’t realize their thyroid is involved until a simple TSH blood test flags it. Once thyroid levels are corrected with medication, ovulation often returns to a regular pattern.
Hyperprolactinemia
This condition involves higher-than-normal levels of prolactin, a hormone usually associated with breastfeeding. Elevated prolactin can suppress the hormones responsible for triggering ovulation, leading to irregular or missed periods. It can be caused by certain medications, pituitary gland issues, or sometimes has no identifiable trigger. Treatment usually involves medication to lower prolactin levels, after which ovulation frequently resumes.
Stress and Lifestyle Factors
Chronic stress affects the hypothalamus, the part of the brain that kicks off the entire ovulation process. High stress levels, poor sleep, and excessive exercise can all delay or suppress ovulation temporarily. This is often seen in women juggling demanding jobs, intense training schedules, or ongoing emotional strain. Making space for rest and recovery can help the body’s hormonal rhythm reset over time.
Obesity and Being Underweight
Body fat plays a direct role in hormone production, so both too much and too little can disrupt ovulation. Excess fat tissue can increase estrogen production in ways that confuse the ovulation signal, while very low body fat can shut down reproductive hormones altogether. Athletes and women with restrictive eating patterns are particularly prone to this. Reaching and maintaining a healthy weight range often helps regulate cycles naturally.
Age-Related Changes
As women age, egg quantity and quality naturally decline, and cycles can become less predictable. This is a gradual process that usually becomes more noticeable after the mid-30s. It doesn’t mean pregnancy isn’t possible, but it may take a bit more monitoring and support. Fertility testing can give a clearer picture of ovarian reserve at any given age.
Symptoms of Ovulation Problems
Irregular or Absent Menstrual Periods
- Cycles shorter than 21 days or longer than 35 days
- Periods that skip months at a time
- Very light or unusually heavy bleeding
- No periods at all for several months
Difficulty Getting Pregnant
Trouble conceiving after a year of regular, unprotected intercourse (or six months if over age 35) is often the first sign that prompts couples to seek evaluation. This doesn’t always mean something is seriously wrong — sometimes it simply points to a timing issue that can be corrected. A fertility specialist can help narrow down whether ovulation is the underlying factor. Early evaluation tends to lead to quicker, simpler solutions.
Changes in Basal Body Temperature
Basal body temperature rises slightly after ovulation due to increased progesterone. Women who track this daily may notice a flat pattern with no clear temperature shift, which can suggest ovulation isn’t occurring. While not a diagnostic test on its own, it’s a helpful and low-cost way to spot patterns before consulting a doctor. Charting over two to three cycles usually gives a more reliable picture than a single month.
Other Hormonal Symptoms
- Unexplained acne or oily skin
- Excess facial or body hair growth
- Sudden hair thinning on the scalp
- Unexplained weight changes
- Milky discharge from the breasts unrelated to breastfeeding
How Ovulation Problems Are Diagnosed
Medical History and Physical Examination
Diagnosis usually starts with a detailed conversation about cycle history, past pregnancies, weight changes, and any related symptoms. A physical exam may check for signs linked to hormonal imbalance, such as excess hair growth or skin changes. This step helps guide which tests are needed next, avoiding unnecessary or repetitive testing. It also gives the doctor context that blood work alone can’t capture.
Hormone Blood Tests
Blood tests typically measure FSH, LH, prolactin, thyroid hormones, and progesterone at specific points in the cycle. These results help identify where in the hormonal chain the disruption is occurring. Timing matters here — some tests need to be done on particular cycle days for accurate results. Your doctor will usually give clear instructions on when to come in for each test.
Ultrasound Evaluation
A transvaginal ultrasound allows the doctor to see the ovaries directly, checking for follicle development and any cysts. It can also assess the uterine lining thickness, which offers clues about hormonal activity. This is a quick, painless outpatient procedure that provides a lot of useful information in a single visit. It’s often repeated at different points in the cycle to track follicle growth over time.
Ovulation Tracking Methods
- At-home ovulation predictor kits (urine-based LH tests)
- Basal body temperature charting
- Cervical mucus monitoring
- Mid-luteal progesterone blood test
Treatment Options for Ovulation Problems
Lifestyle Modifications
For many women, especially those with PCOS or weight-related irregularities, adjusting diet, physical activity, and sleep habits can restore regular ovulation without medication. Even a modest weight change of 5-10% can make a noticeable difference in cycle regularity. Reducing processed sugar and prioritizing consistent sleep also supports hormonal balance. These changes take time, but they often improve results from other treatments too.
Medications to Induce Ovulation
Medications like clomiphene citrate or letrozole are commonly used first-line treatments to stimulate the ovaries to release an egg. These are taken orally over a few days early in the cycle, followed by monitoring through ultrasound or blood tests. Success rates are generally good, and many women conceive within a few treatment cycles. Your doctor will adjust dosage based on how your body responds each month.
Hormone Therapy
When imbalances involve thyroid hormones or prolactin, correcting those levels with targeted medication often restores ovulation on its own. This is usually a simpler, more direct fix compared to fertility-specific drugs. Regular blood tests help track progress and fine-tune dosage over time. Many women see their cycles normalize within a few months of starting treatment.
Surgical Treatment (When Needed)
In select cases, such as certain ovarian cysts or structural issues affecting the ovaries, a minor surgical procedure may be recommended. This is typically considered only after other treatments haven’t worked or when a specific physical cause is identified. Recovery is usually quick, and many women resume normal cycles afterward. Your doctor will always explain exactly why surgery is being suggested before proceeding.
Assisted Reproductive Technologies (ART)
When medication and lifestyle changes aren’t enough, options like IUI (intrauterine insemination) or IVF (in vitro fertilization) can help achieve pregnancy despite ovulation challenges. These methods work well alongside ovulation-inducing medications to improve timing and egg quality outcomes. The right option depends on age, overall health, and how long you’ve been trying to conceive. A fertility specialist can walk you through which approach fits your situation best.
Can Ovulation Problems Be Prevented?
Maintaining a Healthy Weight
Keeping weight within a healthy range supports steady hormone production and reduces strain on the reproductive system. This doesn’t mean chasing a specific number on the scale, but rather finding a sustainable, comfortable weight for your body. Small, consistent habits tend to work better than short-term extreme diets. A doctor or nutritionist can help set realistic, personalized goals.
Managing Stress
Since stress hormones can interfere directly with ovulation signals, building in regular downtime matters more than people often realize. Simple habits like short walks, breathing exercises, or setting boundaries around work can help regulate the body’s stress response. This isn’t about eliminating stress completely, which isn’t realistic for most people, but about managing it consistently. Over time, this can support more predictable cycles.
Regular Health Checkups
Routine visits allow small hormonal shifts to be caught early, before they turn into bigger fertility concerns. Annual checkups that include thyroid and hormone screening are especially useful for women planning a pregnancy in the next few years. This is a simple, low-effort habit with real long-term benefits. It also builds a helpful health history if fertility treatment is ever needed later.
Healthy Diet and Exercise
- Eating balanced meals with adequate protein and healthy fats
- Limiting excess sugar and highly processed foods
- Moderate exercise (30 minutes most days), avoiding overtraining
- Staying hydrated and getting consistent sleep
When to See a Doctor
Warning Signs That Need Medical Attention
If your periods are consistently irregular, absent for more than three months, or accompanied by symptoms like excess hair growth, acne, or unexplained weight changes, it’s worth booking an appointment. These signs don’t always mean something serious, but they’re worth checking rather than waiting out. Catching things early usually leads to simpler, faster treatment. A short consultation can offer real clarity and peace of mind.
Fertility Evaluation Timeline
Couples under 35 are generally advised to see a specialist after a year of trying without success, while those over 35 should consider evaluation after six months. If you already know your cycles are irregular, there’s no need to wait that long — earlier evaluation is usually more helpful. Testing is straightforward and can often be completed within a few appointments. This gives you and your doctor time to plan the right next steps together.
Consulting Dr. N.S. Saradha for Ovulation Problems
If you’re searching for an experienced Infertility Doctor in Saligramam, Dr. N.S. Saradha’s clinic offers a comfortable, easy-to-reach setting for women dealing with Infertility Problems with Ovulation. The clinic is designed to make evaluation and follow-up visits simple, with straightforward scheduling and a calm, private space for consultations. Understanding ovulation disorder patterns takes time and careful listening, and every visit here starts with a real conversation about your cycle history before any tests are recommended.
Conclusion
Ovulation problems are common, well understood by medical science, and in most cases, very treatable. With the right combination of testing, lifestyle changes, and medical support, most women are able to restore regular ovulation or find a path to pregnancy that works for them. If you’ve noticed irregular cycles or are facing difficulty conceiving, an early conversation with a specialist is the simplest next step toward answers.